Seizures and Epilepsy Overview
Seizure types and Classification
Specific Issues
Driving (See Driving and Neurological Disease)
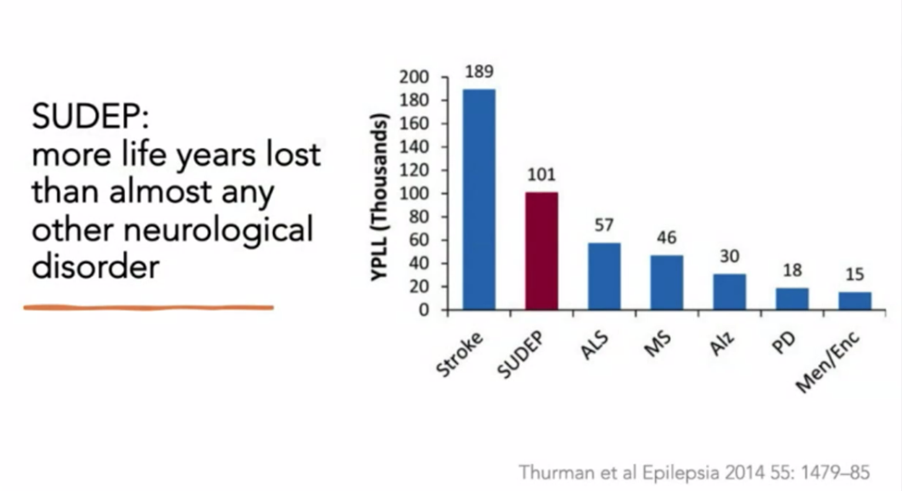
SUDEP (Sudden unexpected death in epilepsy)
Epilepsy and female hormones – menstruation and
menopause
Definitions
Seizure
• The clinical manifestations of an abnormal and excessive excitation of a population of neurons
Epilepsy
• Recurrent seizures which are unprovoked by systemic or neurologic insults
• ILAE – “a disorder of the brain characterized by an enduring predisposition to generate epileptic seizures”
• Requires the “occurrence of at least one unprovoked seizure”
Acute symptomatic seizures (ILAE 2009) - Acute symptomatic seizures
• Seizures occurring in close temporal relationship with an acute CNS insult
• Acute symptomatic seizures differ from unprovoked seizures in risk of seizure recurrence and mortality.
• Seizures are considered acute symptomatic if they occur within the first 7 days of cerebrovascular disease; TBI, including intracranial surgery; CNS infections, multiple sclerosis relapse. Longer timeframes may be appropriate depending on the ‘activity’ of the underlying condition (e.g. a flare of an infectious lesion or a further bleed from an AVM).
• For alcohol withdrawal the seizure must occur within 7–48 h of the last drink.
• Seizures in the setting of a brain tumour may more appropriately classified as epilepsy
Drug resistant epilepsy (ILAE 2009) – replaces term refractory epilepsy
• Failure of adequate trials of two tolerated and appropriately chosen and used AED schedules (whether as monotherapies or in combination) to achieve sustained seizure freedom
Epidemiology
• 5-10%
of the population will have a seizure in their lifetime
• 25-30% due to acute brain disturbance
• 30% of people who ever have a seizure will eventually be diagnosed with epilepsy
Recurrence rate in acute brain disturbance (see below for more details)
• If no structural damage – less than 3%
• If structural damage 12.5% (1/8)
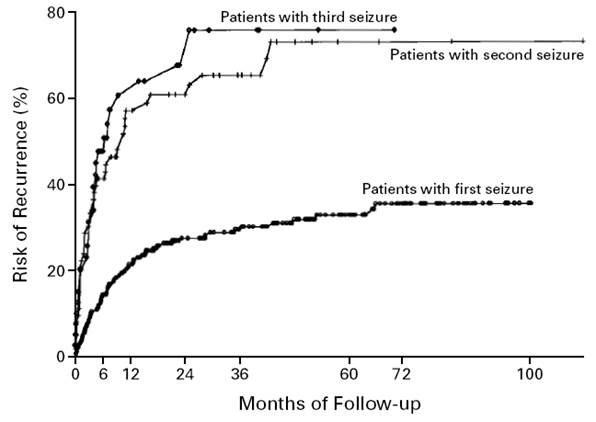
Recurrence rate if unprovoked:
• After one seizure 30-50%
• After 2 unprovoked seizures 70-80% -diagnosis of epilepsy
If a second seizure is to occur 60-70% occur within 6 months
Epilepsy
• Incidence 0.3-0.5%
• Prevalence 0.5-1%
• Lifetime risk 1.4%-3.3%
Seizure types and Classification
Seizure Classification

Focal
• Predominant symptoms at onset
o Use the earliest prominent symptom
o Brief behavioural arrest is common but not used as a descriptor unless it remains the prominent symptom
o The descriptor may not be the most prominent feature of the entire seizure, but the earliest (e.g. starts with prominent but brief automatisms and then has prolonged tonic phase – automatisms would be the descriptor used)
• Focal to bilateral tonic-clonic
o The term secondary generalised was avoided so ensure it was clear that the seizure has a focal onset and the bilateral spread does not have importance in aetiology
• Awareness
o Retained knowledge of self and environment
o Different to responsiveness (which may also be useful to record separately)
o It is noted that there are multiple types of altered consciousness
• Definition
o Originate in networks limited to one hemisphere
o They may be discretely localised or more widely distributed
o They may originate in subcortical structures
Generalised
• Definition
o Originating at some point within and rapidly engaging, bilaterally distributed networks
o The seizure has a consistent focus of onset.
Unknown Onset
• It is suggested that defining the onset as focal or generalised should only be done when there is a >80% chance of certainty
• In many seizures the details surrounding the onset is unknown
• Unknown onset should be used in these circumstances
• Epilepsy syndromes will be grouped according to aetiology (see Epilepsy Syndromes)
|
New Term |
Description |
Old
Term |
|
Hyperkinetic |
Agitated
thrashing or leg pedalling movements |
Hypermotor |
|
Behaviour
arrest |
Arrest
(pause) of activities, freezing immobilization. |
|
|
Cognitive |
Pertaining
to thinking and higher cortical functions. Specific
cognitive impairments Can
be negative: E.g. aphasia, apraxia, neglect, Can
be positive: de ja vu, jamais vu, illusions, halucinations |
Psychic |
|
Epileptic
spasms |
A
sudden flexion, extension or mixed flexion-extensionof
predominantly proximal and truncal muscles that is more sustained than a
myoclonic movement but less sustained than a tonic seizure. Limited forms may occur: grimacing, head
nodding or subtle eye movements.
Frequently occur in clusters. |
Epileptic
spasms |
|
Emotional |
E.g.
Fear, Joy, laughing (gelastic), crying (dacrystic) |
|
|
Clonic |
Jerking,
either symmetric or asymmetric, that is regularly repetitive and involves the
same muscle groups |
|
|
Absence |
Sudden
onset Interruption
of ongoing activities Blank
stare Possible
brief up-ward deviation of the eyes Unresponsive
when spoken to A
few seconds to 30sec Very
rapid recovery (with no post-ictal confusion) |
Absence |
|
Tonic |
A
sustained increase in muscle contraction lasting a few seconds to minutes |
|
|
Myoclonic
|
Sudden,
brief (<100ms) involuntary single or multiple contractions of muscles or
muscle groups. |
|
|
Absence,
atypical |
An
absence seizure with changes in tone that are more pronounced than in typical
absence OR the onset or cessation is not abrupt Often
associated with slow, irregular, generalised spike wave activity |
Absence,
atypical |
Bold text = new ILAE terminology
|
Seizures |
Description |
EEG |
|
Focal |
Localized to discrete area’s of the cerebral
cortex |
|
|
Simple |
Consciousness
maintained “With observable motor
or autonomic symptoms” Motor
Autonomic “With subjective
sensory or psychic symptoms only” = aura Sensory -
Usually numbness or paraesthsia,
visual relatively rare, auditory and vertiginous can also occur -
Olfactory -
Gustatory -
Visceral -
Psychic |
|
|
Complex “With impairment of
consciousness or awareness” = Focal dyscognitive |
Decreased
awareness/ consciousness Automatisms Post-ictal
confusion/amnesia Psychic
symptoms can occur -
Illusions, hallucinations, déjà vu, jamis vu, affective symptoms |
|
|
Partial
with secondary generalization “Evolving to bilateral
convulsive seizure” |
Usually
tonic-clonic seizure |
|
|
Primarily generalized |
Diffuse area’s of the brain simultaneously |
|
|
Tonic-clonic |
May
be vague prodrome Tonic
phase 10-20sec -
Pupils dilated and NR Clonic phase -
8Hz slowing to 4Hz -
~30s -
Ends with deep inspiration Gradually
increasing relaxation Usually
no more than 1min Post-ictal
– unresponsive, flaccid, salivation, bowel/bladder incontinence |
Tonic
phase – progressive increase in generalized low-voltage fast activity
followed by generalized high amplitude, polyspike
discharges. Clonic phase – spike and wave Post-ictal
– generalized slowing. |
|
Absence |
Brief, sudden lapses of consciousness (2-10s)
without lapses of postural control No post-ictal confusion Subtle movements may accompany Usually begin in childhood (4-8yrs) 15-20% of childhood seizures 60-70% resolve during adolescence 50% will also experience TC seizure 33% will have myoclonic jerks |
Generalized, symmetric 3Hz spike and wave
discharge that begins and ends suddenly Hyperventilation provokes seizures and EEG
changes |
|
Typical |
||
|
Atypical |
||
|
With
special features |
Myoclonmic absence Eyelid
myoclonia |
|
|
Myoclonic |
Most
common with metabolic syndromes, degenerative CNS disease, anoxic brain
injury |
Bilateral
synchronus spike and wave pattern – at time of myclonus |
|
Myoclonic atonic |
|
|
|
Myoclonic tonic |
|
|
|
Tonic |
|
|
|
Clonic |
|
|
|
Atonic |
Brief
loss of tone 1-2 sec with loss of consciousness No
post-ictal confusion |
|
|
Unknown |
|
|
|
Epileptic
spasms |
|
|
Clinical features (semiology)
• Focal dyscognitive seizures
o 60% temporal vs 40% extratemporal
By Region:
Temporal lobe - Mesial (limbic)
• FDS evolve relatively gradually (1-2min) and last longer (2-10min) than most extra-temporal seizures
Aura
• Visceral – most common – rising epigastic sensation
• Autonomic – pallor or flushing, BP, HR, pupil size, piloerection
• Cephalic
• Gustatory – taste – usually unpleasant
• Dysmnestic – De ja vu
• Affective - fear
Absence
• Often a prominent feature
Automatisms
• Often ipsilateral to side of seizure
• Dystonic posturing usually contralateral
• Oroalimentary – lip smaking, chewing, swallowing
• Gestural – fumbling, fidgeting, undressing, sexually directed actions
Post-ictal
• Dysphasia – useful lateralizing sign indicating dominant lobe focus
Temporal lobe – lateral
Aura
• Simple auditory phenomena - humming, buzzing, hissing, roaring – superior temporal gyrus
• Olfactory – unpleasant and hard to define – sylvian fissure
• Illusions of size – macropsia, micropsia
• Illusions of weight, distance
• Affective auras rare
Motor activity /Automatisms
• More pronounced, less motor arrest
Frontal lobe
• Frequent, brief attacks with tendency to cluster
• Lack the gradual evolution of temporal lobe seizures
• Some forms only occur from sleep
•
• Motor arrest rare
• Prominent motor signs
o Lower limbs
o Cycling, stepping, kicking
o Can be bizarre, highly excited.
• Head and eye version common
o Head version during full consciousness is useful lateralizing sign of contralateral frontal dorsolateral anterior convexity lesion
• 2014 paper suggests 4 groups:
o Elementary motor signs – posterior frontal lobe
o Elementary motor signs, non-integrated gestural motor behaviour – mid frontal, opercular region
o Integrated gestural motor behaviours, distal stereotypies – frontal pole, mesial anterior cingulate
o Fearful behaviour – anterior mesial, cingulate

Central (peri-rolandic)
• Frequently simple focal seizure (without loss of awareness)
• Contralateral clonic jerking – often with Jacksonian march)
• Bilateral posturing
• Fencing posture – contralateral arm abduction, elevation and flexion with head version to same side – supplementary motor area.
• Sensory symptoms can occur – often followed by jerking movement as seizure spreads anteriorly
• Post-ictal Todd’s paresis common
Parietal
• Aura is common (85%)
• Somatosensory (75%)
o Parietal operculum
• Often multiple aura’s in one patient
• Illusions of body distortion
• Illusion of body parts in space
• Panic attacks/ictal fear
• Ictal pain
• Ictal vertigo
• Mesial parietal
o Recurrent, brief, asymmetrical tonic seizures, rapid recovery
• Intraparietal Sulcus
o Spinning seizures – sense of spinning, turning around while standing, rolling over in bed
• Inferior parietal lobule
o Often temporal like
Occipital
• Visual symptoms
• Elementary visual hallucinations most common – colours, shapes, flashes, patterns
• Complex illusions can occur
• Vision blackouts also common – but often associated with illusions.
Insula
• Anterior
o Abdominal pain
o Gustatory
• Inferior
o Limbic symptoms
• Posterior
o Warmth or pain
o Auditory
• Ref: Lecture at ESA 2018
Cingulate
• Anterior
o Anxiety, Fear
o Hypermotor
• Middle
o Complex movments
• Posterior
o Abdominal aura
o De ja vu
o Hypermotor
o Can be similar to mesial temporal semiology
• Ref: Lecture at ESA 2018
By Symptom:
|
Symptom |
Localisation |
Lateralisation |
Correlation |
|
|
Sensory |
|
|
|
|
|
Well-defined somatosensory symptoms |
Parietal (primary sensory
cortex) |
Contralateral |
High |
|
|
Poorly defined somatosensory symptoms (e.g.
bilateral) |
Parietal (S2 or SMA) |
None |
Low |
|
|
|
|
|
|
|
|
Gustatory Aura |
Insular |
|
|
|
|
|
|
|
|
|
|
Olfactory sensations |
Anterior mesio-
temporal lobe |
None |
|
?Associated with amygdala
lesions |
|
Vertigo |
Insular – parietal – temporal
junction |
None |
? |
|
|
Vertigo –
yaw sensation (spinning around vertical axis) |
Posterior temporal |
|
|
|
|
Vertigo –
spinning around horizontal axis |
Parietal opercular |
|
|
|
|
Ascending visceral feelings |
mesio
– temporal, insular, supplementary motor area |
None press tab moderate |
|
|
|
Unilateral elementary visual phenomena |
Occipital |
Contralateral |
High |
Visual phenomena are often bilateral – which is non lateralising. |
|
Complex
visual hallucinations and illusions |
Parieto-temporal (association cortex) |
None |
? |
|
|
Elementary auditory manifestations (if
unilateral) |
Primary auditory cortex (Heschell’s
gyrus) |
Contralateral |
Low (Lat) |
It is difficult for patients to lateralise sounds. |
|
|
|
|
|
|
|
Déjà vu |
Mesio
temporal |
None |
|
|
|
Ictal fear |
Amygdala |
None |
|
|
|
Orgasmic aura |
Non-dominant mesio temporal or para-sagittal parietal region |
None |
|
|
|
|
|
|
|
|
|
Lateralised ictal headache |
Temporal or occipital |
Ipsilateral |
Moderate |
|
|
Postictal headache |
Non-localising |
|
|
|
|
Pre-ictal headache |
? |
|
|
|
|
|
|
|
|
|
|
Motor |
|
|
|
|
|
Forced head version (Versive seizures) |
Frontal, temporal |
Contralateral |
High |
Versive = eye, head, body movement, forced, sustained unnatural
posture. Probably due to activation of
frontal eye field. Occurs earlier in
frontal lobe seizures. |
|
Non-versive head
turning |
Temporal |
Ipsilateral |
Moderate |
Often will then turn to the contralateral side as the seizure becomes
bilateral TC. |
|
Eye deviation (without head deviation) |
Non-localising |
|
|
|
|
Unilateral
clonic |
Frontal > temporal |
Contralateral |
High (~92% for Lat) |
Frontal clonic – early with preserved
consciousness. Temporal clonic – may occur later, after automatisms. |
|
Unilateral
tonic |
Extratemporal >>temporal |
Contralateral |
High (Lat) |
Generated in cortical motor areas.
Only lateralising if truly unilateral.
|
|
Unilateral dystonia |
Temporal > frontal |
Contralateral |
High |
Dystonic posturing – unnatural tonic posturing with a rotatory
component. |
|
Asymmetric termination of clonic
phase |
Temporal and frontal |
Ipsilateral to the last cloni |
High (80% for Lat) |
|
|
Figure 4
sign (just
prior to BTCS) |
SMA |
Contralateral (to extended arm) |
High (Lat) |
Importantly its significance is limited to the situation where it
occurs just prior to BTCS. |
|
Unilateral
eye blinking |
Unknown |
Ipsilateral (to blinking eye) |
High (Lat) |
Rare |
|
Ictal
Nystagmus |
?Occipital |
Contralateral to fast phase |
? |
|
|
Hand
position |
|
|
|
See Siegel and Tatum. Neurology
Vol 87 2016 |
|
-
Fan |
Onset of GGE TCS |
|
|
|
|
-
Fist |
Tonic and clonic phase of GGE, Clonic phase of FBTCS |
|
|
|
|
-
Index
finger pointing |
Onset of focal epilepsy FBTCS |
|
|
|
|
-
Claw |
Psychogenic events |
|
|
|
|
-
Flaccid |
Psychogenic events |
|
|
|
|
Negative motor phenomena |
|
|
|
|
|
Negative
myoclonus |
Central region |
Contralateral |
? |
|
|
Ictal
akinesia |
|
Contralateral |
High (Lat) |
Different to dystonia which must be excluded Negative motor area’s – anterior to face motor area in frontal lobe |
|
|
|
|
|
|
|
Other |
|
|
|
|
|
Automatisms |
Temporal >frontal |
Ipsilateral |
High |
Often associated with contralateral dystonic posturing – which has the
greater lateralising significance.
Preserved responsiveness during automatisms infers right sided onset. |
|
|
|
|
|
|
|
Ictal speech |
Temporal |
Non-dominant |
High |
Clearly understandable words
or phrases |
|
Autonomic |
|
|
|
|
|
Ictal
urinary urge |
Temporal |
Non-dominant |
? |
|
|
Ictal bradycardia |
Temporal |
None |
|
|
|
Ictal
tachycardia |
Insula |
Non-dominant |
|
|
|
Ictal
piloerection (unilateral) |
Temporal |
Ipsilateral |
? |
Rare (0.14%) |
|
“Cold
shivers”/goosebumbs |
Temporal |
Dominant |
|
(Stefan et al 2002) |
|
|
|
|
|
|
|
Ictal spitting |
Temporal lobe |
Non-dominant |
|
Rare |
|
Ictal
vomiting |
Temporal (+?insula) |
Non-dominant |
|
Often associated with an
epigastric aura |
|
Ictal laughing |
Hypothalamic hamartoma or
temporal or frontal |
- |
- |
|
|
Ictal weeping (dacrystic
seizures) |
Mesio
temporal |
None |
- |
|
|
Peri-ictal water drinking |
Temporal |
Non-dominant |
|
?Incidence up to 15% |
|
Peri-oral myoclonia |
Generalised |
|
|
|
|
Rhythmic Ictal non-clonic
Hand movements (RINCH) – simple movement, not like automatism |
Temporal |
Contralateral |
|
|
|
|
|
|
|
|
|
Post-ictal signs |
|
|
|
|
|
Postictal dysphasia |
Dominant hemisphere |
- |
High |
Must be distinguished from
impaired consciousness |
|
Postictal paresis (Todd’s) |
Temporal or frontal |
Contralateral |
High (Lat) |
Incidence 6-40% |
|
Postictal nose wiping |
Temporal, frontal |
Ipsilateral |
High (Lat 50-97%) |
|
|
Postictal coughing |
?temporal |
Nil |
Mod (Loc) |
Some studies say left,
others right – therefore no clear lateralising value |
* From Rossetti and Kaplan (2010) Seizure semiology; European neurology.
Aetiology
Acute symptomatic seizures
|
|
Risk of
acute seizures |
Risk of chronic seizures |
|
Stroke |
|
|
|
Ischaemic stroke |
2.5-5.0 |
11 |
|
ICH |
16 |
|
|
SAH |
10 |
7 |
|
Infection |
|
|
|
Bacterial
meningitis |
17-24 |
2.7 |
|
Encephalitis |
|
>20 |
|
Cerebral
abscess |
17 |
|
|
Neurocysticercosis |
|
|
|
Cerebral
malaria |
40 |
|
|
HIV |
|
~15% pre- and 6% post
HAART |
|
Inflammatory |
|
|
|
MS |
|
~3x risk, 3.1% at
15years |
|
ADEM |
10-20 |
|
|
SLE |
10-20 |
|
|
Wegener’s |
<5 |
|
|
Bechcet’s |
<5 |
|
|
NMDA
encephalitis |
75 |
|
|
Metabolic |
|
|
|
Hyponatraemia |
5-15 |
|
|
Hypernatraemia |
Rare |
|
|
Liver
failure |
Rare |
|
|
Drugs |
|
|
|
Alcohol
withdrawal |
33 |
|
|
Marijuana |
?Nil |
?Nil |
|
Cocaine |
1-8 |
|
|
Heroin
use |
OR 27 |
OR 4.7 |
|
Ketamine |
?Nil |
?Nil |
|
Head injury |
|
|
|
Closed
|
2-6 |
|
|
Mild |
|
Nil |
|
Mod |
|
1-4 |
|
Severe |
|
10-15 |
|
Open |
|
30-50 |
|
Neurodegenerative diseases |
|
|
|
Alzheimer |
|
6-fold risk |
|
Huntington
disease |
|
5 |
|
CJD |
|
10 |
*Acute symptomatic seizures, Practical Neurology 2012 12:154
Drugs
• Alcohol
• Acute intoxication probably does not cause seizures
• Acute withdrawal – 6-48hours can lower seizure threshold
Medications
|
Drug |
Risk |
|
Anti-psychotics |
All probably have increased risk, listed below
have higher risk |
|
|
|
|
Clozapine |
1-4% |
|
Chlorpromazine |
1-9% |
|
Trifluoperazine |
|
|
Anti-depressants |
Risk ranges from <1-4% |
|
SSRI’s,
MAOI’s |
Lowest
risk |
|
Antibiotics |
|
|
B-Lactams
(Especially - Benzylpenicillin,cephazolin,
imipenem) |
|
|
Isoniazid |
|
|
Quinolones
(ciprofloxacin, norlfoxacin) |
|
|
Other |
|
|
Theophylline |
High |
|
|
|
Tumours
Risk of seizures:
• DNET 80-100%
• Low-grade astrocytoma 75%
• Meningioma 30-60%
• High-grade astrocytoma 30-50%
• Brain metastases 20-35%
• Primary CNS lymphoma 10%
Overall Causes of Seizure
Adults
• Unknown 62%
• Stroke 9%
• Trauma 9%
• Alcohol 6%
• Neurodegenerative disease 4%
• Encephalopathy 3.5%
• Tumours 3%
• Infection 2%
Causes of seizure (by age)
|
Neonates
(less
than 1 month) |
Hypoxia/ischaemia ICH Acute
infection Metabolic Drug
withdrawal Developmental
disorders Genetic
disorders |
|
Infants
and children (1month
to 12 years) |
Febrile
seizures Genetic
disorders CNS
infection Developmental
disorders Trauma Idiopathic |
|
Adolescents (12-18yrs) |
Trauma Genetic Infection Tumour Drug
use Idiopathic |
|
Young
adults 18-35yrs |
Trauma Alcohol
withdrawal Drug
use Tumour Idiopathic |
|
Older
adults Over
35yrs |
Cerebrovascular
disease Tumour Alcohol
withdrawal Metabolic Alzheimer’s/degenerative
disease Idiopathic |
Acute symptomatic seizures
Specific Epilepsy
Syndromes
Patient Evaluation
History
- Previous
seizures including history of febrile seizures
- CNS lesions
- Trauma, CVA,
tumour, vascular malformations
- Prenatal/perinatal
history – i.e. any complications of pregnancy, hypoxia, need for intensive
care.
- Developmental
milestones
- Family
history
- Drug or
alcohol abuse
- Precipitating
factors:
- Sleep
deprivation, systemic disease, electrolyte/metabolic disturbance, acute
infection, drugs – legal/illegal, alcohol.
- Note: OSA
can worsen seizure – think of this if well controlled epileptic worsens
with age
Symptoms:
- Aura’s or
other associated phenomena not previously diagnosed as seizure
- Behaviour
- Vocal
- Motor
- Eyes
- Motionless
stare – MTLE
- Flickering –
absence
- Deviated –
focal
- Rolled back
– syncope
- Closed –
non-epileptic
- Respiration
pattern
- Autonomic –
drooling, pallor, N+V
- LOC
Post ictal
- Amnesia
- Lethargy
- Confusion
- Sleepiness
· Headache
- Muscle ache
- Tongue biting
- Incontinence
- Transient
focal weakness
- N+V
Physical
examination
- Neurological
examination
- Signs of
infection
- Cutaneous
markers of CNS disease
- Signs of
trauma
- Signs of
metabolic disease
- CVS
examination for risk of cerebrovascular disease
Investigations
- Bloods:
- Glucose,
calcium, magnesium, U+E, LFT
- Toxin/drug
screen
- Serum
prolactin
- Lumbar
puncture – if meningitis suspected or HIV pos
Specific Serum Markers of Seizure
• CK
• Prolactin
Ammonia
• Study (2016 Epilepsia 57(8)1228) - 78 patients admitted for VEM for diagnostic purposes
o Ammonia sample taken 15-60min post ictal
o Baseline ammonia was slightly higher in generalised convulsive seizure group
o Significant increase in Ammonia in generalised convulsive seizure group only (not in focal sz or PNES)
o A cut point of >80umol/L gave Sn 53.9% and Sp 100%
EEG
- Abnormal in
29% (range 8 to 50%) of adult patients presenting with first seizure
- Increased incidence
of abnormalities in sleep deprivation
- During event
- Interictal
- 60% are
normal in patients with known epilepsy
Imaging
- CT in
emergency cases, otherwise MRI (although no good evidence)
- A significant
abnormality is present in ~10% of adult patient with first seizure (CT or MRI)
- (Dr Archer)
“80% of significant abnormalities will be detected on CT-B’
Differential diagnoses
- Migraines
- Psychotic
disorders
- TIA/CVA
- Syncope
- Differentiating
from syncope:
|
|
Seizure |
Syncope |
|
Precipitating
|
Usu none |
Stress,
valsalva, cardiac event |
|
Premonitory
symptoms |
None
or aura |
Tiredness,
nausea, sweating, tunnelling of vision |
|
Posture |
Variable |
Usually
erect |
|
Transition
to unconciouness |
Usu.
Immediate |
Gradual
|
|
Duration
of unconsciousness |
Minutes |
Seconds |
|
Duration
of tonic or clonic movt. |
30-60
seconds |
Never
more than 15sec |
|
Facial
appearance during event |
Cyanosis,
frothing at mouth |
Pallor |
|
Aching
muscles after event |
Often |
Sometimes |
|
Biting
of tongue |
Sometimes |
Rarely |
|
Incontinence |
Sometimes |
Sometimes |
|
Headache |
Sometimes |
Rarely |
|
|
|
|
Treatment:
•
Treatment of underlying condition
• Avoidance of precipitating factors
• Anti-epileptic drug therapy
• Avoidance of dangerous activities
• Driving
o Operating machinery or at heights
o Swimming alone
• Treat/screen for concomitant problems
o Depression
• Overall effective in 60-70% of patients
Ketogenic Diet
• Effective, especially in paediatric populations
•
Surgery
• Temporal lobe resections
o 60-70% chance of being seizure free
• Vagal nerve stimulation
o 50% reduction in 30-40% of patients
• Deep brain stimulation
o Under investigation
Refer for surgery when (rule of 2’s):
· 2 years of seizures
· >2seizures/month
· >2monotherapies trialed
· One trial of two drugs combined
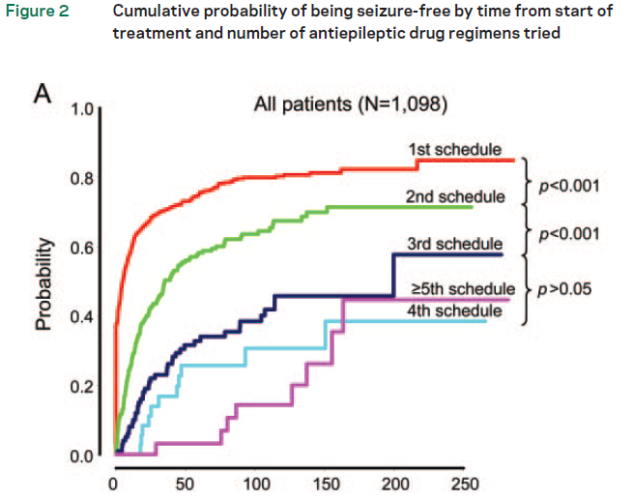
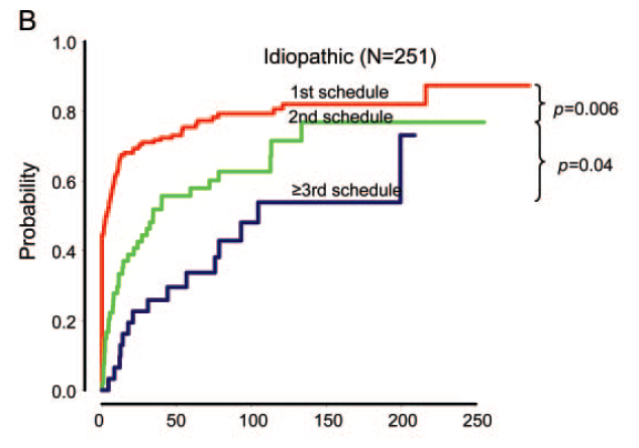
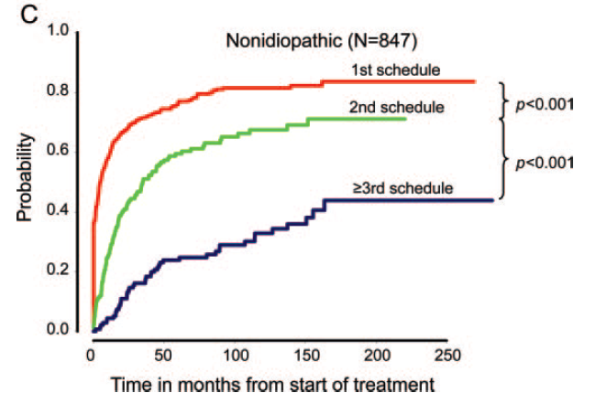
Prognosis with treatment
Patterns of treatment response in newly diagnosed epilepsy,
• Kwan Neurology 2012
• 1098 patients
• Median F/U 7yrs
• Seizure freedom defined as one year
|
Drug Regimens |
% of total cohort Seizure free |
% Seizure free on particular regimen |
% polytherapy |
|
Monotherapy |
49.5 |
49.5 |
|
|
Second |
13.3 |
36.7 |
30.8 |
|
Third |
3.7 |
24.4 |
36.5 |
|
Fourth |
1.0 |
16.2 |
45.5 |
|
Fifth |
0.4 |
12.5 |
75 |
|
Sixth |
0.2 |
12.5 |
50 |
|
Seventh |
0.2 |
22.2 |
50 |
|
Eighth |
0 |
0 |
|
|
Ninth |
0 |
0 |
|
Monotherapy vs polytherapy
• Only 6% of all patients achieved seizure freedom on polytherapy
• Of the occasional successes achieved on latter drug regimens – most were on polytherapy (see table above)
Classified patients into 4 categories/patterns:
|
Pattern |
A |
B |
C |
D |
|
Description |
Becoming and remaining seizure free within 6
months of treatment |
Becoming and remaining seizure free after 6
months of treatment |
Fluctuating between periods of seizure freedom
and relapse |
Never seizure free for any complete year |
|
% |
37% (25% immediately) |
22% |
16% |
25% |
Treatment withdrawal
• Trial in late 1980’s (MRC AED Withdrawal Study Group. Lancet 1991;337:1175-80)
o Patients seizure free for 2 years were randomised to continue treatment or wean and cease
o At 2 years after randomisation seizure freedom was maintained in :
- 78% of patients continuing on medication
- 59% of patients who ceased
o i.e. absolute increased risk of recurrence of 19%, NNT to result in one recurrence = 5.
• Study from China regarding focal epilepsy (Wang et al. CNS drugs 2019, 33; 1121)
o Patients made their own decision regarding cessation – followed for several years
o Chance of remaining seizure free after 5 years depended on how many years the patient had been seizure free prior to medication cessation. Ranging from 39% if seizure free for 2-3years up to 64% if seizure free 5+ years.
• Systematic review and meta-analysis (Lamberink et al. Lancet Neurology 2017, 16:523)
o Devised a decision tool to predict risk of seizure recurrence:
http://epilepsypredictiontools.info/aedwithdrawal
• If a seizure is going to recur 2/3rd will happen within first year
• If seizures occur with medication cessation 95% regained seizure control at 1 year (MRC study)
o Other studies found figures of 76% to 85%
Changing Treatment
• If a patient is seizure free and wishes to change treatment what is the risk of seizure?
o 12 patients changing vs matched controls (Finamore et al. Epilepsia 57(8) 1294 2016)
- 14% excess risk of seizure in next 6 months compared to controls
o Another study suggested 18% (Wang Epilepsia 2012)
Refractory/Drug resistant Epilepsy
· ILAE 2010
o Epilepsy in which seizures persist and seizure freedom is very unlikely to be attained with further AED therapy
o Failure of adequate trial of two tolerated and appropriately chosen and used AED schedules (either as monotherapy or combination) to achieve sustained seizure freedom.
Specific Anticonvulsants
Specific
Issues
Driving
(See Driving
and Neurological Disease)
Epilepsy
and Suicide
- RR = 2 when all
patients with psychiatric disease excluded
- Highest risk
during first half year after diagnosis
- ? common
pathogenic mechanism in terms of receptor abnormalities
SUDEP
(Sudden unexpected death in epilepsy)
Epidemiology
- Australia
~280 deaths/year
- Mean age of
death from epilepsy 52
- Rates
|
|
Per
1000/year |
|
New
onset epilepsy |
~
0.35 |
|
General
population of epilepsy |
~
0.9-2.3 |
|
Refractory
seizures |
~4.0 (1.1-5.9) |
|
Surgery
candidates/failed surgery |
6.3-9.3 |
|
Associated
mental retardation |
~3.0 |
• Incidence seems to be fairly even across age groups (children vs adults)
Pathogenesis
·
Respiratory causes probably important (apnoea seems
to be important common factor)
·
?Cerebral shutdown
·
Small proportion cardiac cause (0.1-0.4% of
seizures observed to cause asystole)
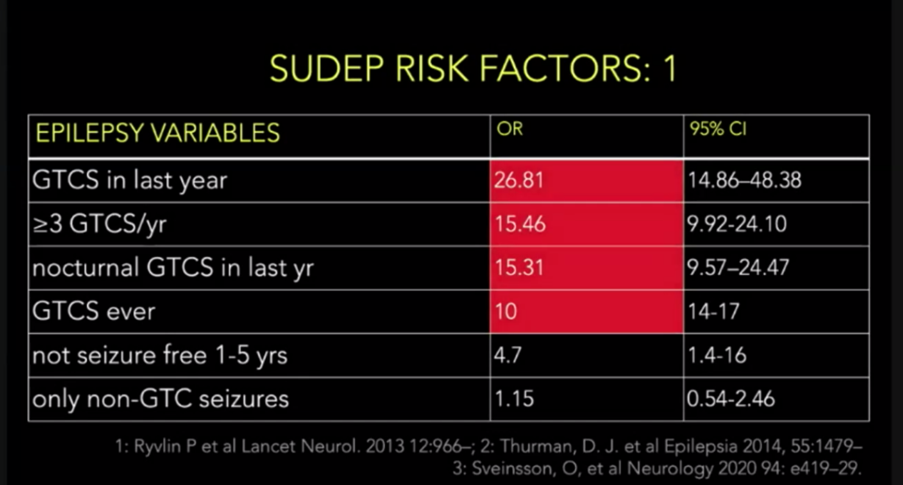
Risk factors
·
Seizures:
o
GTCS
o
Recent or frequent seizures (>3 seizures in last
year ~8x risk)
·
Medications:
o
Non-compliance
o
Recent and frequent changes in medication
o
Patients on polytherapy (polytherapy and
>3seizures ~25x risk)
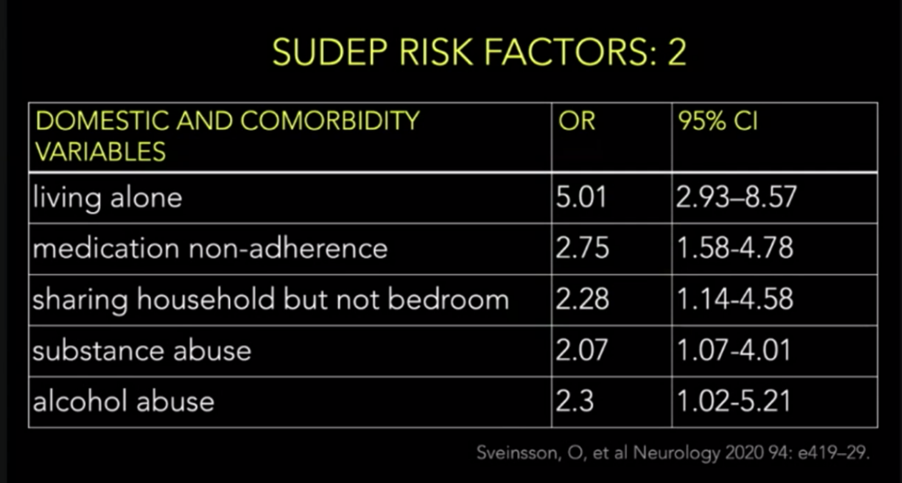
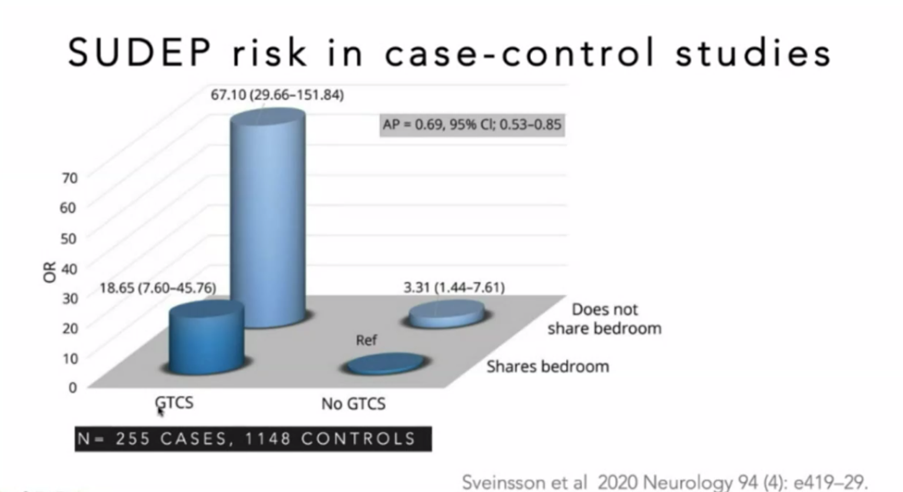
·
Environment
o
?Lack of nocturnal supervision/sleeping alone
·
?Alcohol
·
?Depression
References
- SUDEP NEJM
2011, SUDEP Lancet 2011
- Ryvlin Lancet Neurol 2013
- Thurman
Epilepsia 2014
Epilepsy and Pregnancy
• Fertility
o Equal in young women
o Reduced in older women with epilepsy compared to controls - ?due to decreased desire to have children or ability to have children
• Risk of offspring developing epilepsy
o GGE – offspring have 1/12 chance of inheriting epilepsy (~8%)
o Focal epilepsy – offspring have 1/50 chance (2%)
o Background rate ~1%
• Increased maternal mortality during pregnancy
o 4-7% of all maternal deaths in UK associated with epilepsy
o 10x risk of controls
o Largely SUDEP - ?due to coming off medication due to fear of malformations
• Increased pregnancy complications/morbidity
o 2-4X risk of complications (Haemorrhage, transfusion, preterm delivery)
o Caesarean section increased – Australian pregnancy registry – 39.2% vs 29.9%
• Seizure risk
o Overall 15% of women with epilepsy will have GTCS during pregnancy ?unknown if this is any different from baseline
o 2/3 patients have no change in seizures during pregnancy
- ?1/3 improve, 1/3 stay the same, 1/3 get worse
o However clearly increased risk of seizure during delivery – 2-2.5%
o Reasons for worse seizures during pregnancy:
- Change in metabolism of medication
- Vomiting
- Sleep deprivation
- Withdrawal of medication (due to side effect concerns)
- ?Effect of pregnancy on seizure threshold
• Seizure effect on foetus
o May be a slightly higher rate of spontaneous abortions
o One study shows association with preterm delivery and lower birth weight
o One study demonstrated lower verbal IQ in children with 5 or more TCS during pregnancy
o Vast majority of studies suggest increased seizures DO NOT increase rate of congenital malformation
o Isolated focal seizures unlikely to have any significant impact
•
Discussion
list:
o
Risk
of medications on pregnancy
o
Risk
of seizures on pregnancy
o
Folate
o
Medication
adjustment during and after pregnancy
o
Morning
sickness (redose if vomiting after dose –
recommendations vary from 15-60min after dose)
o
Risk
of seizures peri-partum
-
Avoid
prolonged labour, lower threshold for pain relief
o
Sleep
deprivation
o
New-born
safety
-
Bathing
baby
-
Red
o
Anxiety
and depression
•
Effect
of AEDs – See Anticonvulsants
Epilepsy and female
hormones – menstruation and menopause
Catamenial epilepsy
3 patterns
• C1 during menstruation
• C2 during ovulation
• C3 during anovulatory cycles
• Majority C1
• Trial of progesterone
o Overall no benefit
o Subgroup with C1 may have some benefit
• Old trial (1982) suggested clobazam effective:
o 20-30mg for 10 days starting 2 days prior to usual onset of seizures.
Menopause
• May get better or worse
• More often gets worse in the perimenopause
Seizures from sleep
Studied in WA database
(presented ESA 2015)
• 239 patients with first seizure from sleep (23% of all first seizures)
• 89 patients (40%) eventually developed an awake seizure
• Median onset awake seizure 1.6 years (range 1-12 years)
• 13% risk of seizure in first year drops off substantially thereafter
• After 2 consecutive sleep seizures one year risk of awake seizure is 5%
• After 3 risk is 1.5%
References
“Evaluation of first seizure” Neurology 2007 69:pg1996-2007
“Initial Management of Epilepsy” NEJM 2008 359;2 pg166